 English
English
 Ελληνικά
Ελληνικά What are aqueous drainage devices?
Aqueous drainage devices are used to reduce intraocular pressure by draining the aqueous humor (the fluid which fills the front part of the eye) into a small blister or bleb that forms in the wall of the eye and is covered by the upper eyelid.
The purpose of reducing intraocular pressure is to inhibit the progression of glaucoma. Glaucoma damage to the optic nerve initially leads to loss of peripheral vision and in advanced stages also affects central vision and leads to total blindness.
Aqueous drainage devices are mainly used in cases of extensive glaucoma damage or when the eye has already undergone other anti-glaucoma surgery or other surgery such as vitrectomy, corneal transplantation, etc.
Various drainage devices are available nowadays. The most commonly used are the Ahmed glaucoma valve and the Baerveldt glaucoma implant. In addition, for some time now the Paul implant has been available, which shares technical similarities with the Baerveldt implant.
All devices consist of a small silicone tube (less than 1 mm in diameter) through which the aqueous humor drains into a plate creating a drainage bleb between the eye wall (the sclera) and the superficial sheath covering the eye (the conjunctiva).
The Ahmed glaucoma valve contains a regulating mechanism (a valve) which regulates intraocular pressure and prevents very low pressure (hypotony) in the first weeks after surgery. The Baerveldt implant does not contain a flow control mechanism and therefore we use special sutures in and around the silicone tube to avoid excessive drainage of aqueous humor in the first weeks after surgery. Each of the drainage devices has its own advantages and we can advise on which one is most appropriate for you.
How does the drainage device affect the external appearance of the eye?
In the first days after the operation the eye is red and there is usually swelling of the surrounding area. Both edema and redness subside within the first few weeks after surgery. The drainage device is not normally visible. Sometimes it can be seen only when the eye looks at the extreme gaze positions (eg down and towards the nose) and when we raise the upper eyelid.
When the device is draining normally, the drained fluid forms a blister (bleb) below the conjunctiva and above the device’s plate and from there, the fluid is reabsorbed by vessels on the surface of the eye. Both the device and the blister are covered by the upper eyelid, are not visible and also do not create the feeling of a foreign body. In most cases the device is placed below and behind the upper eyelid. More rarely it can be placed under and behind the lower eyelid.
To keep the device in the correct position and prevent an opening (an erosion) in the surface of the eye that would leave it exposed we use a patch from donor tissue (treated pericardium or eye tissues such as sclera and cornea) which covers part of the device.
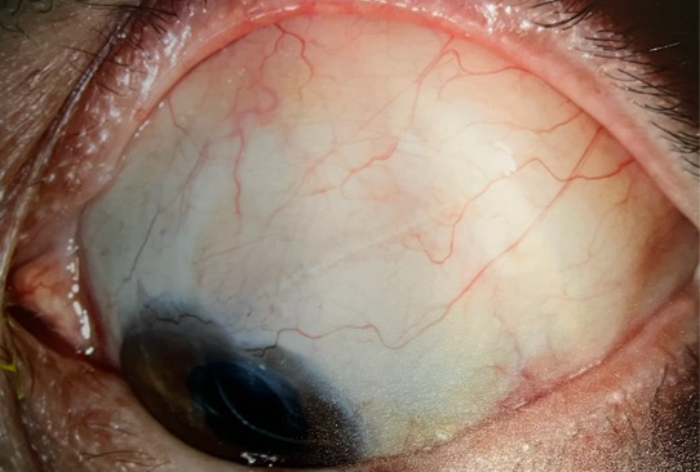
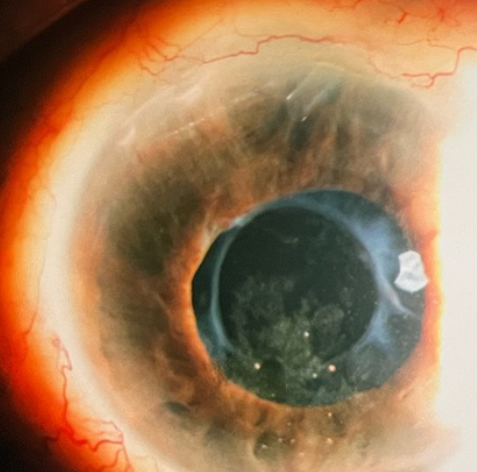
The part of the drainage tube inside the eye is very small, about 1-2 mm and is not visible to the naked eye. The photos show this section at high magnification. The tube is made of transparent silicone, its outer diameter is 0.6 mm and its inner diameter is 0.3 mm.
Most of the time we use a suture to block the inside of the tube and to adjust the pressure in the first postoperative weeks. This suture is removed in the first months after the operation and in case it is colored (blue or black) it can stand out slightly below the conjunctiva when the eye looks at the extreme positions of the gaze.
The surgery
The surgery usually takes one to two hours. It can be done either with general anesthesia or with local anesthesia and sedation. Sometimes we use a drug called mitomycin C which prevents the growth of scar tissue and in addition we cover the implant with a piece of tissue (cornea, sclera or treated pericardium) from donor tissue to prevent possible exposure.
Donor patch
The drainage device is covered with a patch at the point of contact of the sclera with the cornea. Without coverage, the conjunctiva may tear above the device and corrective surgery may be needed. This is observed in a percentage of 10-14% without the use of a patch and in a percentage of only 3% with the use of a patch. The patch is tissue derived from a donor and the tissues we usually use are the cornea or sclera as well as the treated pericardium. The patch is not a living implant and is used to strengthen the surface of the eye. However, as we mentioned, they come from donors and have been previously tested to prevent the risk of transmitting an infectious disease such as syphilis, hepatitis B and C and AIDS. To date it is not possible to test for prion disease (Bovine Spongiform Encephalopathy or BSE, otherwise known as CJD or mad cow disease) as there is no corresponding screening test yet. However, the risk of transmitting this disease seems to be extremely low.
Postoperative Care
You can usually return home the same day or the day after surgery. The eye remains closed with a pad and a plastic shield on the day of surgery. The pad and the plastic shield are removed on the first day after the operation and a postoperative examination is performed. If the other eye has low vision, we can only use the transparent cover without the pad.
Medication – Eye drops
The eye remains closed on the day of surgery and you do not usually need to use drops unless we advise you otherwise. In the other eye you continue to put the drops normally even on the day of the operation.
After removing the pad and the plastic shield on the first postoperative day, we start using two types of eye drops, an antibiotic (usually 4 times a day for at least a month) and an anti-inflammatory steroid. The anti-inflammatory drug is used intensively at the beginning, about 8 times a day and the frequency is gradually reduced in the weeks and months following surgery. In some cases, you continue to use your anti-glaucoma eye drops. We will inform you in detail about the eye drops and the frequency of their use at each postoperative visit.
Postoperative visits
Eye pressure can fluctuate considerably in the first few weeks after surgery. Patients are usually monitored once a week for the first month and then the frequency of visits decreases. Sometimes visits can be more frequent if the pressure is too high or too low.
Intraocular Pressure Fluctuations
In some drainage devices, for example in the Baerveldt device that we use very often, there is no flow restriction mechanism and so we are forced to close the device using sutures (either around the lumen or inside the lumen) to prevent hypotony (very low pressure in the eye). For this reason, the pressure can remain high in the first weeks after surgery. In case the pressure is high we use anti-glaucoma drops as well as diuretic pills (acetazolamide) per os. The sutures around the lumen can be absorbed within the first 6 postoperative weeks or we can remove them using a laser so that the device starts working and the pressure is reduced. The suture inside the lumen is usually removed 3 months after the operation and in some cases maybe even earlier. By removing the suture this device becomes fully functional and the pressure is then well controlled.
Sometimes the pressure can be very low after surgery and this is dangerous for the eye. In this case, we stop the anti-glaucoma treatment and usually reduce the cortisone drops. Sometimes it is necessary to inject gel (viscoelastic) in the anterior chamber of the eye and more rarely to perform corrective surgery to add ligation sutures to the tube, etc.
Activity after surgery
We recommend avoiding strenuous exercise and lifting significant weight in the first 4 to 6 weeks after surgery. Moreover, activities such as yoga or sometime praying with head down postures should be avoided too. If the pressure is too low you may be asked to avoid any activity for a few days and remain sedentary. Activities such as reading and watching TV can be performed without any problems for the operated eye.
Back to work
Returning to work depends on the nature of the work and the postoperative course of the patient. As a general rule, we would say that patients who do office work return to work in 2 weeks as long as the postoperative course is normal while patients who do manual work need at least a month before returning safely.
When does the eye return to normal?
The eye takes about 3 months to return to normal (as before surgery) and sometimes maybe longer if there are complications. Usually after the first trimester we do the check for refraction and the prescription of new glasses as most of the time the prescription changes after the operation.
Success rates and complications
Success Rates
Most studies in glaucoma surgery report success rates in the first 5 years after surgery. From these studies it appears that aqueous drainage devices have a success rate of controlling intraocular pressure between 70 and 80% in the first 5 years. Although they sometimes regulate the eye pressure without the use of anti-glaucoma drops, a large percentage of patients continue to take anti-glaucoma drops so that the pressure is kept low enough. In cases where drops are needed, these are usually fewer than those needed before surgery. In terms of long-term success rates, beyond the five-year period there are no large studies that report success rates. Usually if an aqueous drainage device works properly and controls the intraocular pressure for 5 years, it continues to do so for a long time.
Complications
Serious complications following the insertion of anti-glaucoma devices are uncommon. Serious complications occur if the pressure drops too low or too abruptly in the early postoperative period. In both circumstances, the pressure drop can cause choroidal bleeding (bleeding in the back of the eye). This happens rarely, at a rate of less than 1%. If the pressure is too low after surgery, sometimes we can inject viscoelastic gel or put gas in the anterior chamber of the eye. Rarely does the patient need to re-enter the operating room to adjust the drainage device. Large studies show that about 5% of patients need to return to the operating room in the first month after surgery due to either too low or too high eye pressure.
The risk of infection in the eye after surgery is rare, occurring in less than 1%.
Other possible complications are exposure of the drainage device after erosion of the conjunctiva at the point of coverage and displacement from the initial position which may result in blockage of the tube by the iris or cornea-tube touch. In all these cases corrective surgery is needed. In rare cases of significant damage to the cornea because of cornea-tube touch, corneal transplantation surgery may be necessary.