 English
English
 Ελληνικά
Ελληνικά Minimally invasive glaucoma surgery has been used in recent years and aims to reduce intraocular pressure either by increasing the drainage of the aqueous humor ( the fluid that circulates in the front part of the eye). Included in this section are various procedures that share common features. The approach is generally minimally invasive with small incisions in the cornea and with the least possible trauma to the neighboring tissues, i.e. to the sclera (white wall of the eye) and the conjunctiva (transparent membrane that covers the wall of the eye). They are mainly aimed at patients who have mild or moderate glaucomatous damage or ocular hypertension and can sometimes be combined with cataract surgery.
I-stent
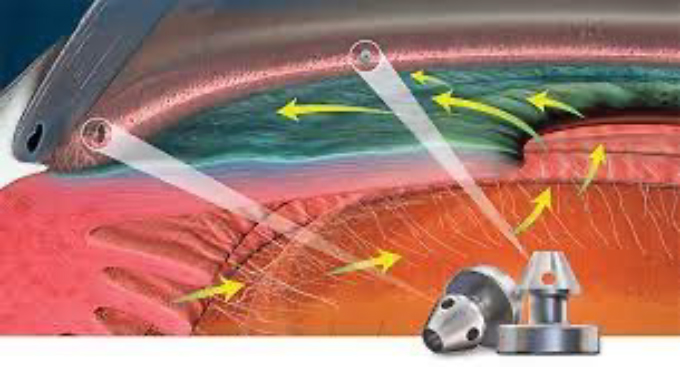
It is a very small tube (about 1 millimeter) which is placed in the normal drainage channel of the eye and increases the drainage of the aqueous humor reducing the pressure as well as the need for anti-glaucoma drops. It is extremely small and is not visible after its placement. It is made of titanium and there is no risk of rejection by the body. In addition, it is compatible with airport scanners as well as MRI scanners.

In which patients can it be used?
The i-stent is suitable for patients who have mild or moderate glaucomatous damage and are about to undergo cataract surgery. It is not suitable for patients with advanced glaucoma, for patients who have high intraocular pressure despite medication and for patients in whom the normal drainage system of the eye has been significantly damaged.
How does it reduce pressure?
The i-stent creates an opening in the eye’s normal drainage channel. This channel malfunctions in glaucoma, obstructs drainage and the pressure rises. Placement of the i-stent overcomes this obstacle, aqueous humor is drained through the opening of the cannula, and the pressure is reduced. It is usually necessary to place 2 stents to achieve the desired result.
What are the benefits?
The placement of the i-stent is fast, technically simple and less invasive than classic anti-glaucoma operations. In a large multicenter study, 2/3 of patients who received an i-stent during cataract surgery had a 20% reduction in pressure and did not require anti-glaucoma therapy compared to ½ of patients who underwent cataract surgery alone (no i-stent).
But the i-stent’s pressure-lowering effect seems to wane over time, and some patients need to restart their medication.
What does surgery involve?
Surgery is usually performed under local anesthesia and mild sedation. Placement of the i-stent takes 5 to 10 minutes and is performed either at the beginning or at the end of the cataract surgery. The i-stent is placed in the normal drainage channel of the eye through a tiny incision and using a placement device. At the end of the surgery, the eye is covered with sterile gauze and a plastic cover. A post-operative examination is needed on the first day after the operation as well as one week later.
What should I expect after surgery?
After surgery the eye may be red and slightly swollen for a few days. Vision gradually improves in the first 1 to 2 weeks. You need to use antibiotics and anti-inflammatory drops and sometimes continue your anti-glaucoma treatment for a while. You can read or watch TV but you should avoid activities like running, swimming, tennis. Most patients can return to work 1 to 2 weeks after surgery.
What are the possible complications?
It is normal to have a little bleeding which subsides a few days after the operation. There is a small risk of the i-stent moving from its original position or its lumen becoming blocked but this is extremely rare. In some cases, the reduction in intraocular pressure may not be enough or last for a short time. If this happens, then you will need to start your anti-glaucoma eye drops again or have another operation to lower the pressure.
Hydrus Microstent
The Hydrus Microstent is a small flexible tube that is inserted into the eye’s natural drainage channel to reduce intraocular pressure as well as the need for medication with eye drops. It is so small that you will not see or feel it after the procedure. The device is made of a super-elastic alloy of nickel and titanium. This material does not cause an allergic reaction and has been used in over a million medical implants. It doesn’t trigger airport scanners and is safe if you need to have an MRI.
In which patients can the Hydrus Microstent be used?
Hydrus is best suited for patients with mild to moderate open-angle glaucoma taking glaucoma drops who are about to undergo cataract surgery and wish to reduce their need for glaucoma medication.
Hydrus is not suitable for patients with advanced glaucoma or in whom the normal drainage system has been significantly damaged.
How does it work;
The tiny Hydrus Microstent is designed to be inserted into the main drainage channel of the eye and opens the channel to allow the blocked fluid to flow more freely, thereby reducing the pressure in the eye.
What are the benefits?
Hydrus helps reduce pressure in the eye and may reduce the need for or dependence on eye drops in patients with mild to moderate glaucoma. The Hydrus insertion process is faster, simpler and less invasive than traditional glaucoma surgery.
After combined Hydrus Microshunt insertion and cataract surgery, 7 of 10 patients were medication-free 2 years after surgery compared with only 3 of 10 patients who had cataract surgery alone.
The Hydrus Microstent does not cure glaucoma, it does not reverse any damage already caused by glaucoma, and it cannot restore any lost vision.
What does the operation involve?
The operation is usually performed under local anesthesia and perhaps mild sedation. The local anesthetic lasts for several hours and may affect your vision during this time.
The Hydrus Microstent is usually implanted at the end of cataract surgery through the same microincisions required for cataract surgery, meaning no additional incisions are required. A special cannula is used to insert the device into the eye’s main fluid drainage channel, called Schlemm’s canal.
At the end of the procedure, we usually close the operated eye with sterile gauze and a plastic cover. Most patients will need to be seen in the first day as well as in the first week after surgery.
How soon will I recover?
After surgery your eye may be slightly red and swollen for a few days. Your vision may also be blurry for 1 – 2 weeks after the procedure. You can read and watch TV as per normal.
You will be given new anti-inflammatory and antibiotic eye drops to prevent inflammation and infection.
The Hydrus Microstent will start working immediately to reduce the pressure in your eyes and you can stop taking the glaucoma drops in the operated eye. Any drops you use in your other eye should be continued as normal.
As with all eye procedures, you should avoid vigorous activity for the first month, including swimming, tennis, jogging and contact sports. Most people take 1 – 2 weeks off after surgery, however the length of time will depend on the nature of your work.
You should avoid wearing eye makeup for about 4 weeks after surgery.
What are the most common complications?
It is normal to have a small amount of bleeding inside the eye during the operation but this subsides within a few days. There is a risk of the Microstent becoming blocked or dislodged, but this is rare.
In some cases, the Hydrus Microstent may not reduce eye pressure or its effect may wear off over time. If the Hydrus Microstent fails to lower your eye pressure, it will not cause additional damage to your eye. However, you may need to restart your glaucoma medications or have further surgery to control your eye pressure.
Preserflo Microshunt
What is Preserflo Microshunt?
The Microshunt is a small 8mm tube that is placed in the eye to reduce intraocular pressure and the need for anti-glaucoma eye drops in patients suffering from glaucoma. It is made of a synthetic and biocompatible material called SIBS. There is no risk of rejection by the body and it is also compatible with airport scanners as well as CT and MRI.
In which patients can it be used?
It is usually used in patients whose intraocular pressure is not adequately controlled with antiglaucoma drops. It has a better hypotonic effect than the other devices belonging to the category of minimally invasive glaucoma surgery (eg I-stent, Hydrus, Trabectome). It is believed that in some cases Microshunt may have similar efficacy to trabeculectomy and thus may be used as a first antiglaucoma procedure in patients suffering from moderate glaucomatous damage who have not previously undergone glaucoma surgery.
How does the Microshunt work?
The Microshunt is placed in the anterior chamber of the eye and drains the aqueous humor by forming a bleb (a liquid reservoir) under the conjunctiva (the transparent membrane that covers the eye wall). Unlike minimally invasive surgical devices that facilitate drainage through the normal drainage channel of the eye (eg, I-stent, Hydrus, Trabectome), the Microshunt creates a bypass drainage pathway. It is not visible except under a microscope.
What are the benefits?
Microshunt effectively reduces intraocular pressure and inhibits the progression of glaucomatous damage. The results are comparable to those of trabeculectomy but the Microshunt operation is shorter, less invasive and requires fewer post-operative checks. In addition, the bleb created after Microshunt placement is usually smoother and less elevated than the trabeculectomy bleb and thus allows the use of contact lenses postoperatively.
What does surgery involve?
Surgery is usually performed under local anesthesia and mild sedation. As with trabeculectomy, we use an anti-healing drug called mitomycin. We make a small incision in the conjunctiva (the transparent membrane that covers the white of the eye) and place the Microshunt through an extremely small incision in the anterior chamber of the eye. Then we close the opening in the conjunctiva with stitches (usually 2 or 3) which are removed later or absorbed by themselves. The duration of the operation is 30-45 minutes.
What should I expect after surgery?
After surgery the eye may be red and slightly swollen for a few days. Vision gradually improves in the first 1 to 2 weeks. You need to use antibiotics and anti-inflammatory drops. We usually use the antibiotic 4 times a day for 1 month and the anti-inflammatory 4 to 6 times in the beginning and reduce the frequency until we stop it about 3 months after the operation. The reduction in pressure after Microshunt placement is immediate, so you should stop ALL anti-glaucoma drops you were taking before surgery. You can read or watch TV but you should avoid activities like running, swimming, tennis. Most patients can return to work 1 to 2 weeks after surgery.
What are the possible complications?
Serious complications are very rare. It is normal to have a little bleeding which subsides a few days after the operation. If bleeding occurs vision may be slightly blurred for 1 to 2 weeks.
As with all other anti-glaucoma procedures, the hypotonic effect of Microshunt can weaken over time. This occurs due to the development of scar tissue resulting in reduced drainage of the aqueous humor. If the drainage of the aqueous humor decreases and the pressure rises, you will need to start your antiglaucoma treatment again or have a new surgery. As with other procedures that create a drainage bleb, with the Microshunt there is a small risk of infection in the eye as well as a very small risk of exposure of the cannula through the conjunctiva. If the cannula is exposed, corrective surgery is needed to cover it again and prevent possible infection. Finally, there is always a risk that the pressure will drop too low, but this risk is significantly lower than with trabeculectomy. Even if the pressure is significantly reduced in the first days after the operation, it usually returns to normal levels without need for another surgery.
Το χειρουργείο γίνεται συνήθως με τοπική αναισθησία και ήπια μέθη. Όπως και κατά την τραμπεκουλεκτομή, χρησιμοποιούμε ένα αντι-επουλωτικό φάρμακο που ονομάζεται μιτομυκίνη. Κάνουμε μια μικρή τομή στον επιπεφυκότα ( τη διαφανή μεμβράνη που καλύπτει το λευκό του ματιού) και τοποθετούμε το Microshunt μέσω μιας εξαιρετικά μικρής τομής στον πρόσθιο θάλαμο του ματιού. Στη συνέχεια κλείνουμε το άνοιγμα στον επιπεφυκότα με ράμματα ( συνήθως 2 ή 3) τα οποία αφαιρούνται αργότερα ή απορροφούνται μόνα τους. Η διάρκεια της επέμβασης είναι 30-45 λεπτά.
Τι να περιμένω μετά το χειρουργείο;
Μετά το χειρουργείο το μάτι μπορεί να είναι κόκκινο και ελαφρώς πρησμένο για κάποιες μέρες. Η όραση βελτιώνεται σταδιακά στις πρώτες 1 με 2 εβδομάδες. Χρειάζεται να χρησιμοποιείτε αντιβιοτικές και αντιφλεγμονώδεις σταγόνες. Συνήθως χρησιμοποιούμε το αντιβιοτικό 4 φορές τη μέρα για 1 μήνα και το αντιφλεγμονώδες 4 με 6 φορές στην αρχή και μειώνουμε τη συχνότητα ως που το σταματάμε 3 μήνες περίπου μετά την επέμβαση. Η μείωση της πίεσης μετά την τοποθέτηση Μicroshunt είναι άμεση και έτσι θα πρέπει να σταματήσετε ΟΛΕΣ τις αντιγλαυκωματικές σταγόνες που λαμβάνατε πριν την επέμβαση. Μπορείτε να διαβάσετε ή να δείτε τηλεόραση αλλά θα πρέπει να αποφεύγετε δραστηριότητες όπως το τρέξιμο, το κολύμπι, το τένις. Οι περισσότεροι ασθενείς μπορούν να επιστρέψουν στην εργασία τους 1 με 2 εβδομάδες μετά την επέμβαση.
Ποιες είναι οι πιθανές επιπλοκές;
Οι σοβαρές επιπλοκές είναι πολύ σπάνιες. Είναι φυσιολογικό να υπάρξει μια μικρή αιμορραγία η οποία απορροφάται λίγες μέρες μετά την επέμβαση. Αν υπάρξει αιμορραγία η όραση μπορεί να είναι ελαφρώς θολή για 1 με 2 εβδομάδες.
Όπως συμβαίνει και με όλες τις άλλες αντιγλαυκωματικές επεμβάσεις έτσι και η υποτονική δράση του Microshunt μπορεί να εξασθενήσει με το χρόνο. Αυτό συμβαίνει εξαιτίας της ανάπτυξης ουλώδους ιστού με αποτέλεσμα να μειώνεται η αποχέτευση του υδατοειδούς υγρού. Αν η αποχέτευση του υδατοειδούς υγρού μειωθεί και η πίεση ανέβει, θα χρειαστεί να ξεκινήσετε ξανά την αντιγλαυκωματική σας αγωγή ή να κάνετε μια καινούρια χειρουργική επέμβαση. Όπως και με τις άλλες επεμβάσεις που δημιουργούν μια φυσαλίδα αποχέτευσης έτσι και με το Microshunt υπάρχει ένας μικρός κίνδυνος μόλυνσης στο μάτι καθώς και πολύ μικρός κίνδυνος έκθεσης του σωληνίσκου διαμέσου του επιπεφυκότα. Αν ο σωληνίσκος εκτεθεί χρειάζεται διορθωτική επέμβαση ώστε να καλυφθεί εκ νέου και να προλάβουμε πιθανή λοίμωξη. Τέλος, υπάρχει πάντα ο κίνδυνος η πίεση να πέσει σε πολύ χαμηλά επίπεδα αλλά ο κίνδυνος αυτός είναι σημαντικά μικρότερος σε σχέση με την τραμπεκουλεκτομή. Ακόμη και αν η πίεση μειωθεί σημαντικά τις πρώτες μέρες μετά την επέμβαση, συνήθως επανέρχεται σε φυσιολογικά επίπεδα χωρίς την ανάγκη διορθωτικού χειρουργείου.